When you pick up a prescription at the pharmacy, you might not realize that the drug you get isn't just chosen by your doctor - it's also filtered through a hidden system called a preferred generic list. These lists are the backbone of how health insurers decide which medications to cover at the lowest cost. And if you've ever been surprised by a $15 copay for a pill that used to cost $180, you've already felt the impact of these lists in action.
How Preferred Generic Lists Work
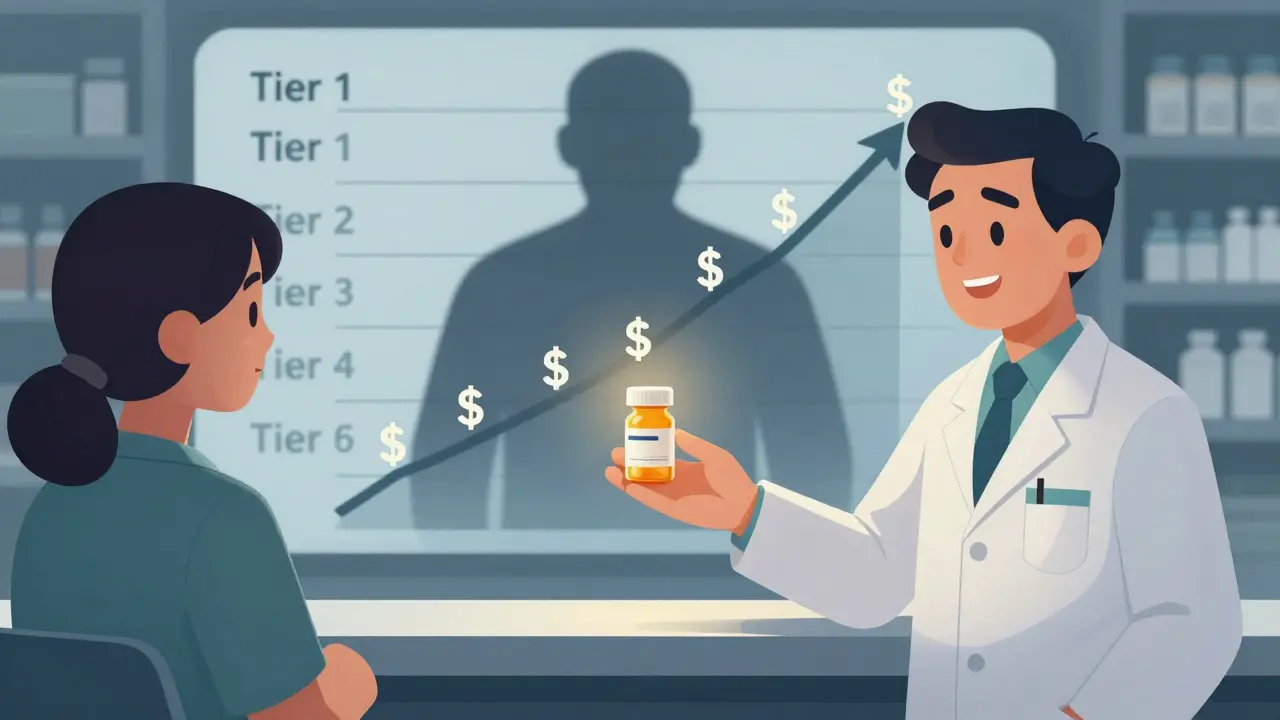
Insurers don’t just pick drugs at random. They use tiered formularies - essentially ranking systems - to steer patients toward the most cost-effective options. The lowest tier, Tier 1, is almost always reserved for preferred generic drugs. These are FDA-approved copies of brand-name medications that work the same way but cost 80-85% less. In some cases, when six or more generic versions of a drug are on the market, prices can drop by as much as 95%.
For example, levothyroxine, a thyroid medication, has dozens of generic versions. One patient on Reddit reported switching from the brand-name version to a generic and cut their monthly cost from $187 down to just $12. That’s not luck - it’s how the system is designed.
The tiered structure usually looks like this:
- Tier 1: Preferred generics - $5 to $15 copay
- Tier 2: Preferred brand-name drugs or higher-cost generics - $25 to $50 copay
- Tier 3: Non-preferred brand-name drugs - $50 to $100 copay
- Tier 4: Specialty drugs (like biologics) - $100+ or coinsurance
Medicare Part D plans and 98% of commercial insurance plans use this structure. The goal isn’t to deny care - it’s to make sure the most affordable, equally effective options are used first. And it works. In 2023, 90% of all prescriptions filled in the U.S. were for generics, even though those drugs made up only 23% of total drug spending.
Why Insurers Push for Generics
It’s simple math. Insurance companies pay for prescriptions through Pharmacy Benefit Managers (PBMs) - middlemen that negotiate drug prices with manufacturers. PBMs get rebates and discounts, especially on generics. In fact, they often buy generics directly from manufacturers at deep discounts, cutting out the middleman entirely. That’s why a generic statin might cost $10 at your pharmacy while the brand-name version is $150.
When a drug has multiple generic competitors, the price keeps dropping. A 2022 FDA report showed that drugs with six or more generic versions can cost 95% less than the original brand. That’s billions in savings for insurers - and those savings get passed on to you in lower premiums and copays.
But it’s not just about price. Formularies are built by panels of doctors and pharmacists who review clinical data. The FDA requires generics to match brand-name drugs in strength, dosage, and how they’re absorbed by the body. Studies show that 98.5% of approved generics meet this standard. So when your insurer says a generic is preferred, it’s not because they’re cutting corners - it’s because it’s just as safe and effective.
The Hidden Trade-Offs
There’s a catch. Not all drugs are created equal - especially biologics. These are complex, injectable medications used for conditions like rheumatoid arthritis, Crohn’s disease, or psoriasis. Brand-name biologics like Humira can cost over $1,200 a month. Their cheaper copies, called biosimilars, are available now - but insurers often don’t put them on Tier 1.
Why? Because brand-name manufacturers offer co-pay assistance programs that cover the entire out-of-pocket cost. Biosimilar makers don’t - and insurers can’t. So even though a biosimilar might cost $850 instead of $1,200, if you were getting $1,200 in co-pay help before, now you’re stuck paying the full $850. That’s a net loss for the patient, even if the list price is lower.
That’s why 44% of patients on biologics report trouble switching to preferred biosimilars, according to Cigna’s 2023 member survey. And it’s why only 15% of eligible biologic prescriptions in the U.S. switch to biosimilars - compared to 85% in Europe.

Step Therapy and Other Barriers
Insurers don’t just prefer generics - they sometimes require you to try them first. This is called “step therapy.” You might have a doctor who says you need a brand-name drug because of your medical history. But your insurer says: “Try the generic first.”
The American Medical Association found that 42% of physicians have seen delays in treatment because of step therapy - especially in chronic pain or mental health cases. One patient described waiting six weeks for a prior authorization to get back on their original medication. By then, their condition worsened.
But here’s the thing: 68% of these denials get overturned when your doctor submits documentation showing why the generic won’t work for you. It’s not impossible - it just takes effort.
What You Can Do
You don’t have to accept what your insurer says without question. Here’s how to take control:
- Check your formulary every year. During open enrollment, review your plan’s drug list. If your medication is on Tier 3 or 4, see if a generic alternative exists on Tier 1.
- Ask your pharmacist. In 89% of states, pharmacists can swap a brand-name drug for a generic unless your doctor specifically says “dispense as written.” Most patients don’t know this - but your pharmacist does.
- Appeal denials. If your drug is denied, your doctor can submit a letter explaining why it’s medically necessary. The Kaiser Family Foundation found that 68% of appeals succeed.
- Use tools like GoodRx or Medicare’s Plan Finder. GoodRx’s 2023 survey of 15,000 patients found that 76% saved money using generics - but 63% hit roadblocks like prior authorizations. Knowing your options helps you push back.
Patients who spend just 45 minutes a year reviewing their formulary reduce their medication costs by 32%, according to SmithRx’s 2023 study. That’s not a small win - it’s hundreds of dollars saved.
The Bigger Picture
The U.S. generic drug market hit $122.7 billion in 2023. PBMs processed 5.8 billion prescriptions - 89% of them generics. CVS Health, Cigna, and UnitedHealth control 78% of this market. That’s why formularies are so powerful: they’re not just clinical tools. They’re economic engines.
But change is coming. Starting in 2025, Medicare Part D will be required to place biosimilars in the same tier as the brand-name drugs they copy. That should push biosimilar use from 15% to 45%. And new “value-based formularies” are being tested - where tier placement isn’t just about price, but real-world outcomes. Will that mean better care? Or just more complexity?
One thing’s clear: insurers prefer generic lists because they work. They save money. They don’t sacrifice safety. And when used right, they help patients too. But the system isn’t perfect. It’s built on cost - not always on compassion. And if you don’t understand how it works, you might pay more than you should.
Why do insurers only cover certain generics?
Insurers don’t cover all generics - only the ones they’ve negotiated the best prices for. A drug might have 10 generic versions, but the insurer only picks the top 2 or 3 that give them the deepest discounts. These become "preferred" generics. Others are left off the list or moved to higher tiers where you pay more.
Can I ask my doctor to prescribe a brand-name drug instead of a generic?
Yes - but your insurer may deny coverage unless your doctor explains why the generic won’t work for you. This is called a "medical exception" or "prior authorization." If your doctor writes "dispense as written" on the prescription, that helps. Still, you may end up paying the full cost if the insurer won’t cover it.
Are generic drugs really as good as brand-name ones?
For most drugs, yes. The FDA requires generics to be bioequivalent - meaning they deliver the same amount of medicine into your bloodstream as the brand-name version, within a 80-125% range. Studies show 98.5% of approved generics meet this standard. For common conditions like high blood pressure or cholesterol, generics work just as well. But for drugs with narrow therapeutic windows - like warfarin or seizure medications - some doctors prefer to stick with the brand, even if it costs more.
Why do biosimilars cost less but I still pay more?
Brand-name biologic manufacturers often offer co-pay cards that cover your entire out-of-pocket cost. Biosimilar makers don’t - and insurers can’t offer them either. So even though a biosimilar might cost $850 instead of $1,200, if you were getting $1,200 in co-pay help before, now you pay the full $850. That’s a net increase in cost for you, even if the list price is lower.
How often do insurers change their preferred drug lists?
Insurers update their formularies at least once a year - often more. A drug might be on Tier 1 this year, then move to Tier 3 next year if a cheaper generic enters the market or if the insurer renegotiates pricing. That’s why checking your plan’s formulary during open enrollment is critical. You might find your medication suddenly costs more - or suddenly becomes much cheaper.
Final Thoughts
Preferred generic lists aren’t a conspiracy. They’re a practical, data-driven system that saves the U.S. healthcare system $1.68 trillion a year. But they’re also a system built for efficiency - not always for ease. If you’re on a chronic medication, don’t assume your insurer has your best interest at heart. Know your formulary. Ask questions. Push back. And remember: the lowest price isn’t always the best value - but the best value is often hiding in plain sight.
William Minks
March 7, 2026 AT 06:06phyllis bourassa
March 7, 2026 AT 20:54Amina Aminkhuslen
March 8, 2026 AT 09:32Susan Purney Mark
March 9, 2026 AT 02:56Ian Kiplagat
March 9, 2026 AT 15:41Jeff Mirisola
March 11, 2026 AT 06:44Bridget Verwey
March 11, 2026 AT 14:28amber carrillo
March 11, 2026 AT 23:52Weston Potgieter
March 12, 2026 AT 08:32Andrew Poulin
March 13, 2026 AT 17:18Adebayo Muhammad
March 15, 2026 AT 00:32Pranay Roy
March 15, 2026 AT 14:07Tim Hnatko
March 16, 2026 AT 13:16