
Imagine waking up to find your lips look like they've been stung by a swarm of bees or your tongue feels too large for your mouth. There is no itch, no hives, and no obvious reason for the sudden change. For someone taking blood pressure medication, this isn't just a weird skin reaction-it could be a life-threatening emergency. ACE Inhibitor Angioedema is a sudden, severe swelling of the deeper layers of the skin and submucosal tissues, often affecting the face, lips, and airway. Unlike a typical allergic reaction, this specific drug reaction doesn't respond to the usual emergency treatments like Benadryl or EpiPens, making it a dangerous trap for both patients and doctors who aren't looking for it.
| Attribute | Detail |
|---|---|
| Incidence Rate | 0.1% to 0.7% of users |
| Primary Cause | Accumulation of Bradykinin |
| High-Risk Groups | African Americans, Women |
| Typical Onset | Often within the first week, but can occur after years |
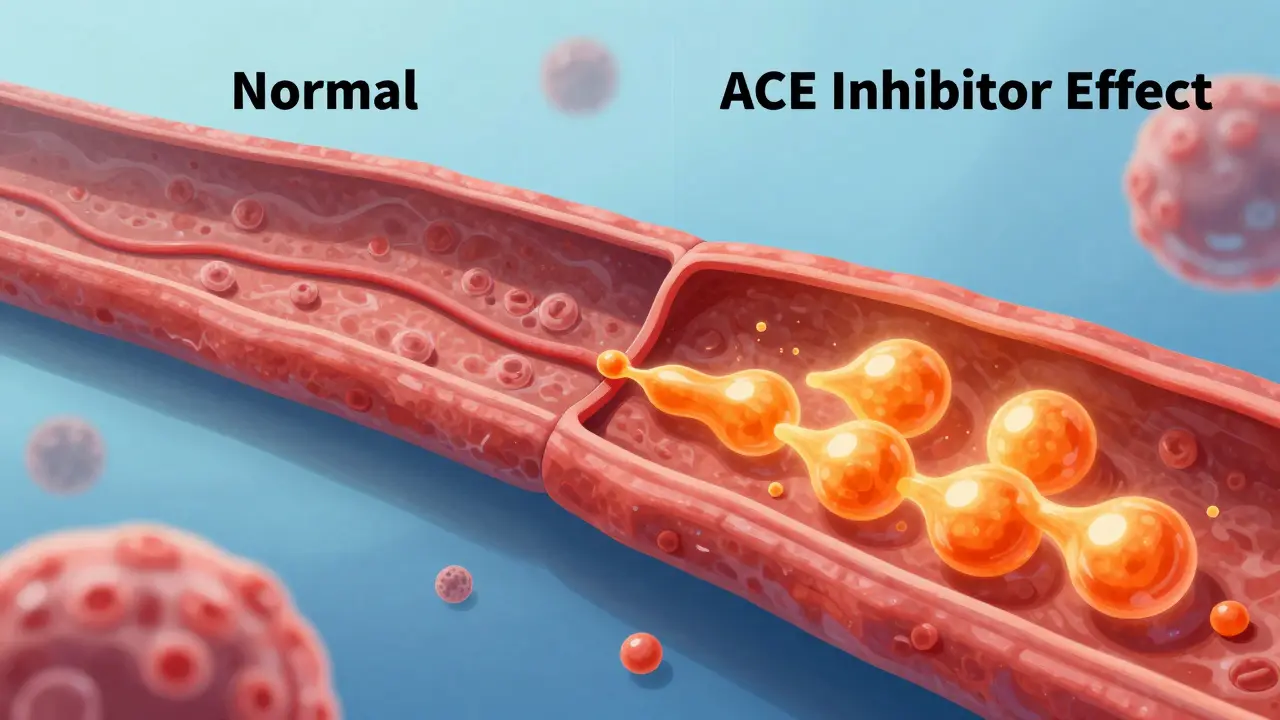
Why This Swelling Is Different From a Normal Allergy
Most people associate swelling with allergies. When you're allergic to peanuts or bee stings, your body releases histamine, which causes hives and itching. But ACE Inhibitor Angioedema is a different beast entirely. It is driven by Bradykinin is a potent vasodilator peptide that causes blood vessels to leak fluid into surrounding tissues.
Normally, the Angiotensin-Converting Enzyme (ACE) is an enzyme that helps regulate blood pressure and breaks down bradykinin in the body handles the cleanup. When you take an ACE inhibitor to lower your blood pressure, you're blocking that enzyme. If your body can't find another way to clear the bradykinin-perhaps due to a genetic quirk in your XPNPEP2 gene-the peptide builds up. This leads to vascular leakage and that signature swelling.
Because histamine isn't the culprit, standard allergy meds are useless. If a doctor gives you epinephrine or steroids for this reaction, it simply won't work. This is a critical distinction because wasting time on the wrong treatments can allow the swelling to reach the throat, cutting off your airway.
Recognizing the Warning Signs
The onset of this reaction is often unpredictable. While about half of the cases happen within the first week of starting a new prescription, others are true sleepers. There are documented cases of people developing this reaction after ten years of taking the same pill every morning without a single issue. This unpredictability is why you can't assume you're "safe" just because you've been on the drug for a while.
Watch for these specific signs:
- Sudden swelling of the lips, tongue, or cheeks.
- A feeling of fullness or tightness in the throat.
- Difficulty swallowing or a change in your voice (sounding muffled).
- Swelling that occurs without itching or hives.
If you notice any of these, the clock is ticking. Swelling in the face often migrates toward the larynx (voice box). If you start struggling to breathe, it's an absolute emergency.
Who Is Most at Risk?
While anyone taking these meds can react, some populations are hit harder. Research from the NIH shows that African Americans have a 2 to 4 times higher risk of developing this reaction than other groups. Women are also affected more frequently, with a reported ratio of about 2:1 compared to men.
There is also a dangerous drug interaction to be aware of. If you are taking an ACE inhibitor for your heart and a DPP4 Inhibitor is a class of oral hypoglycemic agents used to treat type 2 diabetes for diabetes, your risk of angioedema jumps significantly-potentially 4 to 5 times higher than if you were only taking the blood pressure medication.

Immediate Steps and Long-Term Management
If you suspect you are having a reaction, the most important action is the most simple: stop taking the medication immediately. Continuing to take the drug can lead to more frequent and severe episodes. However, don't just stop your blood pressure meds without a plan, as rebounding hypertension can also be dangerous. Contact your doctor instantly to transition to a new therapy.
In an emergency room setting, the priority is airway protection. If the throat is closing, doctors may need to perform intubation. Once the airway is safe, they may use specialized treatments. One such drug is Icatibant is a bradykinin B2 receptor antagonist that blocks the effects of bradykinin to reduce swelling , which can provide relief within a few hours. Some clinicians may also use Fresh Frozen Plasma (FFP) off-label to provide the missing ACE enzyme needed to clear the bradykinin.
For the future, you must avoid all medications in the ACE inhibitor class. This includes common drugs like Lisinopril, Enalapril, and Captopril. Many doctors will switch patients to Angiotensin II Receptor Blockers (ARBs) is a class of medications that lower blood pressure by blocking the action of angiotensin II, but without interfering with bradykinin breakdown . ARBs have a much lower risk of causing swelling-about 10 times lower-though a small percentage of people (10-15%) may still experience cross-reactivity.
Preventing Future Mistakes
A huge problem in healthcare is how this reaction is recorded. If a medical chart simply says "allergy to Lisinopril," a different doctor might think you just had a mild rash and prescribe another ACE inhibitor like Ramipril. This can be fatal.
To protect yourself, ensure your medical records explicitly state "ACE Inhibitor-Induced Angioedema" as a permanent contraindication. This tells any provider that the entire class of drugs is off-limits. Given that only about 42% of patients receive proper counseling on this permanent avoidance, the responsibility often falls on the patient. Wearing a medical alert bracelet is a highly recommended move, especially for those who have had severe airway episodes.
Why don't antihistamines work for ACE inhibitor swelling?
Standard allergy medications like Benadryl or epinephrine target histamine. However, ACE inhibitor-induced angioedema is caused by the buildup of bradykinin, not histamine. Because the biological trigger is different, the medications designed to stop histamine have no effect on the swelling caused by bradykinin.
Can this happen if I've been taking the medicine for years?
Yes. While many reactions occur in the first week, about 20% of cases happen after prolonged use. There are documented instances of patients developing angioedema after a decade of stable therapy. You are not "immune" to the reaction just because you've taken the drug for a long time.
Is it safe to switch to an ARB?
Generally, yes. Angiotensin II Receptor Blockers (ARBs) do not interfere with the breakdown of bradykinin, making them a much safer alternative. However, about 10-15% of people who reacted to ACE inhibitors may still experience cross-reactivity with ARBs, so a transition should be monitored closely by a physician.
How long does the swelling take to go away?
Acute symptoms usually resolve within 24 to 48 hours after stopping the medication. However, some people report mild swelling episodes that linger or recur for several months after the drug has left their system.
What should I do if my tongue or lips start swelling?
Seek emergency medical attention immediately. Because this swelling can progress rapidly to the upper airway and cause suffocation, you should not wait to see if it goes away on its own. Inform the emergency staff immediately that you are taking an ACE inhibitor.
Vijay AGarwal
April 25, 2026 AT 00:41Absolute nightmare scenario! Imagine the sheer panic of feeling your own throat closing up while the doctors are blindly pumping you full of steroids that do absolutely nothing because they don't realize it's bradykinin! It's a literal race against time!
Anand Mehra
April 26, 2026 AT 19:15classic medical gaslighting waiting to happen. system fails and then we wonder why
Kristen O'Neal
April 27, 2026 AT 07:22This is so important to highlight. I wonder if there are better ways to flag this in electronic health records so a different doctor doesn't accidentally prescribe another ACE inhibitor just because the chart says "allergic to Lisinopril" without the specific reason.
Andre Ojakäär
April 27, 2026 AT 14:58everyone knows lisinopril is a gamble lol. honestly just go to an ARB and stop pretending this is some rare medical mystery. it's literally textbook stuff
Eric Mwiti
April 28, 2026 AT 01:45Oh great, so we just trust that 42% of doctors actually tell us about this. Truly top-tier healthcare right here.
Majestic Blue Band
April 29, 2026 AT 22:09It is completely suspicious that these specific medications are pushed so aggressively by the pharmaceutical giants when they know full well about these risks, and honestly, I suspect that the 'bradykinin' explanation is just a convenient cover for something more sinister, perhaps a way to keep us dependent on more expensive ARBs that they've patented in a more lucrative way, because if you actually look at the timing of these releases, it all lines up too perfectly to be a coincidence and the fact that we are told to just wear a bracelet as if that's a real solution to a systemic failure of medical transparency is just laughable.
sachin singh
May 1, 2026 AT 20:27The information regarding the interaction with DPP4 inhibitors is particularly illuminating and provides a necessary caution for those managing both hypertension and diabetes simultaneously.
Gauri Parab
May 2, 2026 AT 05:43Please, let's not pretend this is some revolutionary discovery. Any first-year med student knows about bradykinin accumulation. The real issue is the mediocrity of general practitioners who can't distinguish a histamine response from a peptide-mediated one. It's honestly embarrassing that we even need articles to explain this to the masses.
Elle Torres Sanz
May 2, 2026 AT 08:29It's so vital to look out for our communities, especially knowing that African American patients face a significantly higher risk. We should be encouraging everyone to advocate for themselves and their families in the clinic.
Michael Chukwuma
May 3, 2026 AT 05:49That sounds terrifying. I'm glad there's a safer alternative like ARBs for people who go through this.
Beena Garud
May 3, 2026 AT 11:51One must contemplate the fragility of the human biological system, where a single enzyme's inhibition can lead to such a catastrophic failure of the respiratory gateway. It is a stark reminder of our inherent vulnerability.
suresh kumar
May 5, 2026 AT 10:49Total chaos in the veins! Just imagine your face ballooning up like a giant red pufferfish while you're trying to order a coffee. Absolute madness!
Karyn Tindall
May 6, 2026 AT 11:01The thought of waking up and not being able to breathe because of a pill you've taken for years is just haunting!
Edwin Perez
May 7, 2026 AT 06:30Big Pharma just swaps one drug for another and calls it a cure. Same cycle, different pill.
William Zhigaylo
May 8, 2026 AT 19:51Your insistence on calling this a 'cycle' is an insult to the pharmacological rigor required to develop ARBs. It is a matter of molecular specificity, not a corporate conspiracy. Learn the science before posting your ignorance.