
Imagine looking at a sunny day and suddenly seeing a dark shadow creep across your vision. It feels like someone is slowly closing the blinds on one side of your world. This isn't just a bad headache or tired eyes. This could be retinal detachment, a condition where the light-sensitive layer at the back of your eye pulls away from its supportive tissue. If you ignore it, you could lose your sight permanently. But if you act fast-really fast-you can save your vision. Time is literally the most critical factor here. Every hour that passes without treatment reduces your chance of full recovery by about 5%. So, knowing what to look for and understanding how surgeons fix this problem isn't just medical trivia; it’s a safeguard for your future ability to see.
Recognizing the Warning Signs Before It’s Too Late
The retina is like the film in an old camera. If it detaches, the image gets blurry or disappears entirely. The good news? Your body usually sends clear distress signals before total vision loss occurs. You need to know these six specific warning signs inside out.
- Sudden increase in floaters: These are small dark spots or squiggly lines drifting across your field of view. A few occasional floaters are normal as we age. But if you suddenly see "a shower" of new ones appearing within hours, that’s a red flag. The National Eye Institute notes that patients often describe this as a sudden clouding of vision.
- Flashes of light (photopsias): You might see brief flashes of lightning-like streaks, especially in your peripheral vision. These happen when the vitreous gel inside your eye tugs on the retina. While common during normal aging, persistent flashes combined with other symptoms indicate potential tearing.
- A dark curtain or shadow: This is arguably the most urgent sign. Patients often describe it as a gray curtain being drawn across their vision, starting from the side and moving inward. NYU Langone Health ophthalmologists call this the definitive symptom requiring immediate attention.
- Sudden blurry or distorted vision: About 68% of cases involve noticeable changes in clarity. Straight lines might look wavy, or text might become unreadable. Cleveland Clinic data shows this distortion often accompanies the initial tear.
- Loss of peripheral vision: According to the Retina Research Foundation, 73% of patients report losing side vision. You might bump into doorframes or miss cars in your blind spot because part of your visual field has gone dark.
- Changes in color perception: When the macula-the central part of the retina responsible for sharp, detailed vision-is affected, colors may appear washed out or different than usual.
If you experience any combination of these, do not wait until morning. Do not check online forums first. Go to an emergency room or contact a retina specialist immediately. As Dr. Carl Regillo, Chief of Retina Service at Wills Eye Hospital, emphasizes, "every hour counts." Delaying treatment beyond 72 hours drops the chance of regaining good vision from 75% down to just 35%.
How Doctors Diagnose Retinal Detachment
When you arrive at the hospital, the goal is speed and accuracy. General practitioners often misdiagnose early symptoms as simple eye strain, leading to dangerous delays. That’s why you need a dilated fundus examination, which is considered the gold standard for diagnosis.
Here’s what happens during the diagnostic process:
- Dilated Fundus Examination: The doctor puts drops in your eyes to widen your pupils. They then use a special magnifying lens called an indirect ophthalmoscope (typically a 20D or 30D lens) to look deep into the back of your eye. This allows them to see tears, holes, or areas where the retina has lifted.
- B-Scan Ultrasonography: Sometimes, blood or cataracts block the view of the retina. In these cases, doctors use ultrasound waves to create an image of the eye’s interior. The ODC Accutome B-scan system is commonly used to detect detachments even when direct visualization isn’t possible.
- Optical Coherence Tomography (OCT): This non-invasive scan provides high-resolution cross-sectional images of the retina. It helps determine the exact location and extent of the detachment, particularly useful for assessing macular involvement.
Specialized equipment like the Haag-Streit slit lamp biomicroscope ensures precise evaluation. Remember, general ophthalmologists miss up to 22% of early detachments compared to retinal specialists who have only a 5% error rate. If you’re unsure whether your provider has access to these tools, ask specifically about their capability to perform dilated exams and ultrasonography.
Surgical Options: How Surgeons Reattach the Retina
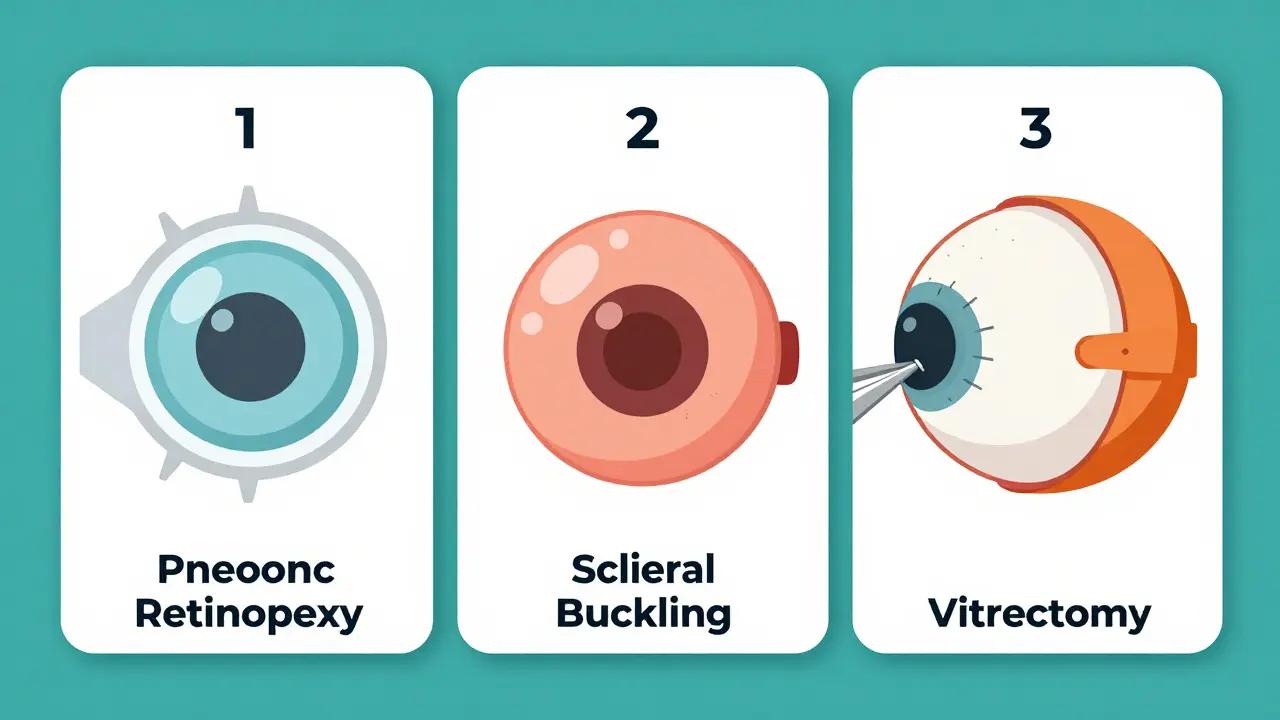
Once diagnosed, surgery is almost always necessary. There is no medication that will reattach a detached retina. The choice of procedure depends on the type, size, and location of the break, as well as your overall eye health. Here are the three primary surgical approaches currently used by vitreoretinal specialists.
| Procedure | Success Rate | Best For | Key Risks/Considerations |
|---|---|---|---|
| Pneumatic Retinopexy | 70-80% | Single, superior breaks in phakic eyes | Requires strict face-down positioning; contraindicated for inferior breaks |
| Scleral Buckling | 85-90% | Young patients with lattice degeneration | Induced myopia (-1.5 to -2.0 diopters); diplopia risk (5-8%) |
| Vitrectomy | 90-95% | Complex detachments, PVR, giant tears | Accelerates cataract formation (70% within 2 years) |
Pneumatic Retinopexy involves injecting a gas bubble into the eye. The bubble floats up and pushes the retina back against the wall of the eye. Laser or freezing therapy then seals the tear. This is less invasive but requires you to keep your head positioned precisely so the bubble stays in place. It’s not suitable for all types of breaks.
Scleral Buckling is an older technique that remains highly effective. The surgeon places a silicone band around the outside of the eye to indent the wall, relieving tension on the retina. It preserves the natural lens longer than vitrectomy, making it attractive for younger patients. However, it can change your prescription significantly and sometimes causes double vision.
Vitrectomy is the most common approach today, accounting for 65% of cases according to the American Society of Retina Specialists. The surgeon removes the vitreous gel pulling on the retina and replaces it with a gas bubble or silicone oil. This offers the best anatomical success rates for complex cases, including those involving proliferative vitreoretinopathy (PVR). The trade-off is a high likelihood of developing cataracts sooner if you still have your natural lens.
What to Expect During Recovery
Recovery from retinal detachment surgery is not like recovering from LASIK. It demands patience, discipline, and often significant lifestyle adjustments. One of the biggest challenges is positioning. If you had pneumatic retinopexy or vitrectomy with a gas bubble, you must keep your face down for 50 to 24 hours a day for 7 to 10 days. Yes, face down. This keeps the bubble pressing against the retina while it heals.
This requirement is difficult. Forty-one percent of patients report significant discomfort, and 38% need home health assistance during this period. You’ll likely sleep in a recliner chair rather than a bed. Friends and family should prepare to help with cooking, cleaning, and childcare during this window.
Other postoperative considerations include:
- No flying: If you have a gas bubble in your eye, air travel is strictly prohibited until the bubble dissolves. Cabin pressure changes can cause the bubble to expand dangerously, spiking intraocular pressure.
- Cataract progression: If you undergo vitrectomy and still have your natural lens, there’s a 70% chance you’ll develop a cataract within two years. Many patients plan for subsequent cataract surgery.
- Elevated eye pressure: About 25% of patients experience temporary spikes in intraocular pressure, which may require eye drops to manage.
- Recurrence risk: Despite successful surgery, 5-15% of patients may experience another detachment, depending on the technique used and underlying conditions.
Visual improvement doesn’t happen overnight. Even after successful reattachment, it can take weeks or months for vision to stabilize. Some permanent loss of peripheral vision may remain, especially if the macula was detached for more than a few days.

Who Is at Highest Risk?
Understanding your risk profile helps you stay vigilant. Retinal detachment affects approximately 1 in 10,000 people annually in the general population. However, certain groups face much higher odds:
- High myopia: People with severe nearsightedness (greater than -5.00 diopters) have a 167 in 10,000 annual incidence rate. The elongated shape of the eye stretches the retina, making it thinner and more prone to tears.
- Post-cataract surgery patients: Having had cataract surgery increases your lifetime risk to between 0.5% and 2.0%. The change in eye structure alters vitreous dynamics.
- Lattice degeneration: This thinning of the peripheral retina affects about 1% of the population and carries a significant lifetime risk of detachment.
- Previous eye trauma: Blunt force injuries can cause immediate tears or weaken the retina over time.
- Family history: Genetics play a role, particularly in conditions like Stickler syndrome.
If you fall into any of these categories, regular dilated eye exams are non-negotiable. Don’t skip them because you feel fine. Retinal problems often have no symptoms until they become emergencies.
Emerging Technologies and Future Outlook
The field of retinal surgery is evolving rapidly. Minimally invasive vitrectomy systems like the EVA Platform, approved by the FDA in January 2023, use 27-gauge instruments that reduce surgical trauma and speed up recovery. Intraoperative OCT guidance is becoming standard, improving the completeness of membrane removal by 15% according to recent studies.
Looking ahead, bioengineered retinal patches are currently in Phase II clinical trials (NCT04872981), offering hope for more durable repairs. AI-assisted screening tools are predicted to reduce diagnostic delays by 30% within five years, potentially preserving photoreceptor function through earlier intervention. While current surgical methods remain highly effective-with vitrectomy utilization increasing 22% from 2018 to 2023-these innovations promise better outcomes with fewer complications.
Despite technological advances, the fundamental rule remains unchanged: early detection saves sight. The global market for retinal treatments continues to grow, driven by aging populations and improved accessibility. However, disparities persist, with only 35% of US counties having access to retinal specialists. Advocating for timely care and understanding your own risk factors are the most powerful tools you have.
Is retinal detachment painful?
No, retinal detachment itself is typically painless. The main symptoms are visual disturbances like floaters, flashes, and shadows. Pain may occur after surgery due to inflammation or elevated eye pressure, but the detachment event does not hurt. This lack of pain is dangerous because people often delay seeking help, thinking it’s not serious.
Can retinal detachment heal on its own?
No, retinal detachment cannot heal on its own. Once the retina separates from the underlying tissue, it loses its blood supply and begins to die. Without surgical intervention to reattach it, permanent vision loss is inevitable. Early surgery offers the best chance for restoring functional vision.
How long does it take to recover from retinal detachment surgery?
Physical healing takes several weeks, but visual stabilization can take months. Most patients need to maintain specific head positions for 7-10 days post-surgery. Full recovery varies based on the procedure type, whether the macula was involved, and individual healing rates. Follow-up appointments are crucial to monitor progress and address complications like cataracts or elevated pressure.
What is the difference between a retinal tear and retinal detachment?
A retinal tear is a hole or rip in the retina, while retinal detachment occurs when fluid passes through that tear and lifts the retina away from the back of the eye. All detachments start with tears or breaks, but not all tears lead to detachment. Treating a tear with laser or cryotherapy can prevent it from progressing to a full detachment.
Does insurance cover retinal detachment surgery?
Yes, most major insurance plans, including Medicare and Medicaid, cover retinal detachment surgery as it is considered medically necessary. Average reimbursement ranges from $3,850 for office-based procedures to $7,200 for operating room surgeries. Coverage details vary by plan, so verify benefits with your provider beforehand, but financial concerns should never delay emergency care.
Aishwarya Thankachan
June 7, 2026 AT 14:44OMG this is literally terrifying 😱👀 I just had a massive spike in floaters yesterday and thought it was just eye strain from coding all night. The part about the 'shower' of new ones appearing within hours? That sounds EXACTLY like what happened to me last week! 🌧️💥 I’m so glad I read this before ignoring it. My optometrist said it’s probably just vitreous syneresis but now I’m paranoid about that dark curtain thing 🚩📉. Does anyone else feel like their eyes are constantly betraying them after reading medical articles?? 🤯🙈
Jerry Mathews
June 8, 2026 AT 12:45Hey Aishwarya, take a deep breath! It’s totally normal to feel anxious after reading something like this, especially when your body gives you weird signals. But remember, not every floater means disaster. If you’ve already seen an optometrist and they cleared you, try to trust that assessment for now. Just keep an eye out for those specific red flags mentioned in the post-like the sudden shadow or flashes-and if anything changes, go back immediately. You’re doing the right thing by being informed and proactive. Stay calm and take care of yourself! 👍😊
Lenny Cruz
June 9, 2026 AT 04:40The article presents a rather pedestrian overview of retinal pathology, failing to adequately address the nuanced biomechanical stresses involved in high myopia cases. While the statistical data provided is ostensibly accurate, it lacks the critical depth required for a truly sophisticated understanding of vitreoretinal interface dynamics. Most laypeople simply do not grasp the intricate relationship between axial length elongation and retinal thinning, which is the primary driver here. Furthermore, the emphasis on emergency room visits is somewhat misguided; one should seek a dedicated retina specialist immediately, as general practitioners are woefully unequipped to handle such delicate matters with the precision required. It is amusing how many people still believe a quick glance through a slit lamp is sufficient for diagnosis.
Aswin Narayan J
June 10, 2026 AT 11:06Listen up, you lot. This isn't some soft science mumbo-jumbo. Retinal detachment is a hard fact, not a suggestion. In India, we see this daily because people ignore the symptoms until it's too late. They think it's just 'eye fatigue' from staring at screens. Wrong. Dead wrong. If you have high myopia, you are sitting on a ticking time bomb. Don't wait for the curtain to fall. Go get your eyes checked. Now. Not tomorrow. Today. Stop making excuses and start taking responsibility for your health. It's that simple.
Jonathan Paul
June 12, 2026 AT 09:22i mean, isnt the whole concept of 'saving sight' just another way society pressures us to conform to visual norms? like, why do we need perfect vision anyway? maybe losing peripheral vision is a spiritual journey into the darkness within ourselves. but whatever, i guess if you want to keep your precious eyeballs working, you gotta do the surgery. just dont forget that true enlightenment comes from within, not from some gas bubble in your eye lol. also, did u know that staring at the sun can actually help reset your circadian rhythm? just saying. dont @ me.
Roderick Gooden
June 12, 2026 AT 13:18I must say, while I generally agree with the urgency portrayed in this piece, I find myself compelled to elaborate extensively on the nuances of the surgical recovery process, which is often glossed over in such brief summaries. The requirement for face-down positioning, particularly following pneumatic retinopexy or vitrectomy with a gas bubble, is not merely an inconvenience but a profound test of human endurance and discipline, demanding a level of commitment that few are truly prepared for without adequate psychological preparation and support systems in place. One cannot simply underestimate the physical toll this takes on the cervical spine and the mental fortitude required to maintain such an unnatural posture for extended periods, often leading to significant discomfort and sleep deprivation that can exacerbate the overall stress of the situation. Moreover, the social isolation experienced during this period, where one is unable to engage in normal activities or even look at others in the eye comfortably, adds another layer of complexity to the recovery journey that is rarely discussed in clinical literature but is deeply felt by patients and their families alike. Therefore, it is imperative that we consider these holistic aspects of care when advising patients, ensuring they are fully equipped to handle the multifaceted challenges that lie ahead.
ANGELA CHINENYE
June 12, 2026 AT 18:10To clarify, the distinction between a retinal tear and a full detachment is critical. A tear is a break in the tissue; a detachment is the separation caused by fluid passing through that break. Treating the tear early with laser photocoagulation or cryotherapy can prevent the detachment entirely. This is a key point often missed. Regular dilated exams are essential for high-risk individuals, specifically those with high myopia or a history of cataract surgery. Do not delay screening. Early intervention preserves photoreceptor function. The statistics cited regarding the 5% hourly decline in recovery chances are accurate and underscore the necessity of immediate action upon symptom onset. Please consult a retina specialist promptly if you experience any of the listed symptoms.
Francis Saul
June 14, 2026 AT 03:42hey guys, just wanted to add that its really important to listen to your body. if u see flashes or floaters, dont ignore it. i had a friend who waited too long and lost a lot of vision. its scary but better safe than sorry. hope everyone stays healthy!
Dave Villeneue
June 15, 2026 AT 08:41The efficacy of scleral buckling is frequently overstated in modern contexts. Vitrectomy remains the superior modality for complex cases due to higher anatomical success rates. Patients exhibiting non-compliance with postoperative positioning protocols should be deemed unsuitable candidates for pneumatic retinopexy. Diagnostic accuracy hinges on specialized equipment availability. General practitioners lack requisite expertise. Immediate referral to retina specialists is mandatory upon presentation of classic triad symptoms. Delay constitutes negligence.