
Nocebo Effect & Statin Tolerance Calculator
Is Your Pain Real or Psychological?
Based on the SAMSON trial data, up to 90% of perceived statin side effects may be driven by expectation (the nocebo effect). This tool helps assess factors influencing your experience.
Imagine taking a pill that lowers your cholesterol but makes your muscles ache so badly you have to stop. Now imagine that the pain wasn't caused by the drug's chemistry at all, but by your own brain expecting it to happen. This isn't science fiction; it is the reality for millions of people who abandon life-saving heart medication every year. The phenomenon is called the nocebo effect, and when it comes to statins, it might be the biggest obstacle to good heart health.
We often think of side effects as purely chemical reactions. If a drug hurts you, the molecule is doing the hurting. But new research flips this script. It suggests that for most people who quit statins due to muscle pain or fatigue, the culprit isn't the medicine-it is their expectation of harm. Understanding this distinction could mean the difference between a healthy heart and a preventable stroke.
The Science Behind the Sensation: What Is the Nocebo Effect?
To understand why you feel pain from a harmless sugar pill, we need to look at how the brain processes information. The placebo effect is famous: believing a treatment works can make you feel better. The nocebo effect is its dark twin. When you expect negative outcomes-like reading about muscle pain in a drug insert-your brain can actually generate those symptoms. It releases stress hormones and heightens sensitivity to normal bodily sensations, turning a slight twinge into debilitating pain.
In the context of statin therapy, which involves drugs like atorvastatin or rosuvastatin used to lower LDL cholesterol, this effect is surprisingly powerful. Statins are among the most prescribed medications globally, yet up to 50% of potential cardiovascular benefits are lost because patients stop taking them early. Why? Because they believe they are experiencing side effects. The brain, primed to expect trouble, interprets everyday fatigue or minor muscle stiffness as drug toxicity, creating a self-fulfilling prophecy of illness.
The SAMSON Trial: Proof That Expectation Shapes Reality
If the idea sounds controversial, the data is hard to argue with. The breakthrough came from the SAMSON trial, formally known as the Self-Assessment Method for Statin Side-effects Or Nocebo study. Led by researchers at Imperial College London, this was not just another survey. It was a rigorous, 12-month crossover study involving 60 participants who had previously quit statins because of severe side effects.
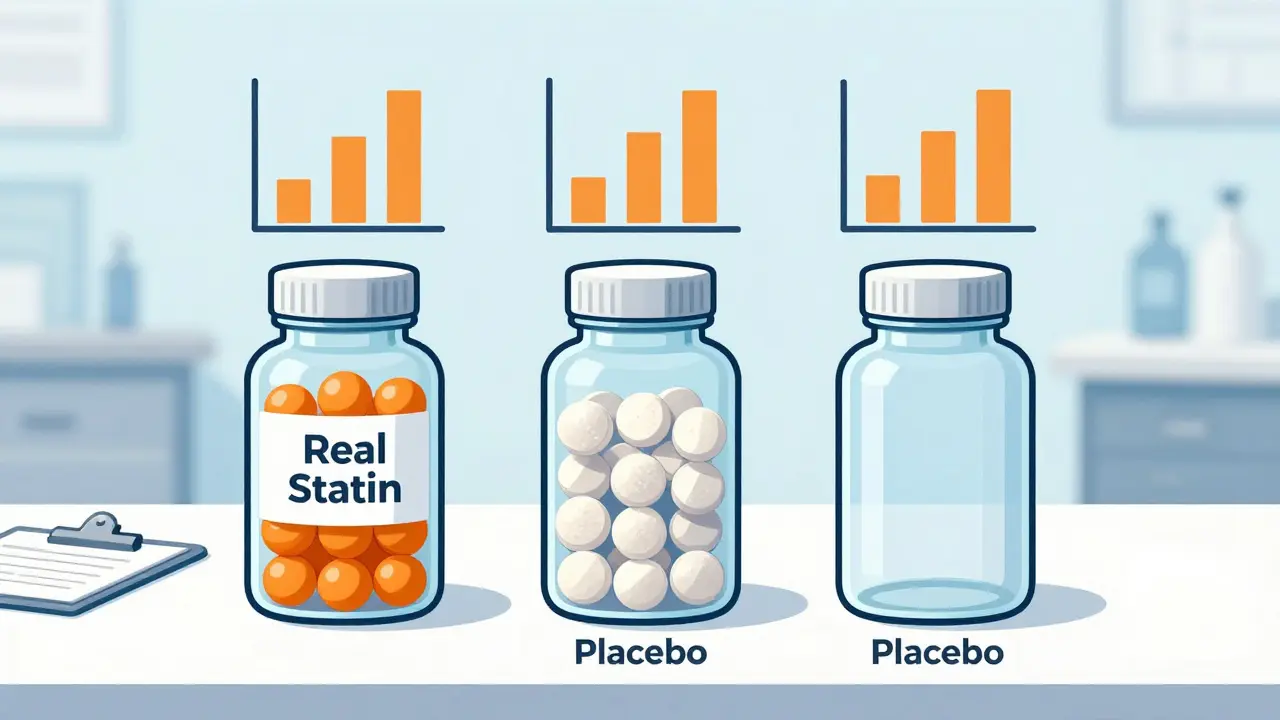
Here is what made the study unique. Each participant received 12 bottles of pills over the year. Four contained actual atorvastatin (20 mg), four contained placebo pills (sugar), and four were empty bottles with no tablets at all. The sequence was randomized, meaning neither the patient nor the doctors knew which bottle was which at any given time. Participants tracked their daily symptom intensity using a smartphone app on a scale of 0 to 100.
The results were striking. During the months when patients took no tablets at all, their average symptom score was 8.0. When they took the placebo, the score rose to 15.4. When they took the real statin, it was 16.3. Crucially, there was no statistically significant difference between the placebo and the statin groups. The calculated "nocebo ratio" was 0.90. In plain English, 90% of the symptoms people blamed on statins were equally present when they were taking fake pills. The pain was real to them, but the cause was psychological, not pharmacological.
| Condition | Average Symptom Score (0-100) | Interpretation |
|---|---|---|
| No Tablet | 8.0 | Baseline background noise |
| Placebo Pill | 15.4 | Symptoms induced by expectation |
| Atorvastatin 20mg | 16.3 | No significant increase vs. placebo |
Perception vs. Reality: How Common Are True Side Effects?
It is vital to clarify that this does not mean everyone’s pain is "fake." The symptoms reported by patients in the SAMSON trial were genuine experiences of discomfort. However, the source was different than assumed. True pharmacological side effects from statins, such as objectively diagnosed myopathy (muscle damage) or rhabdomyolysis (severe muscle breakdown), are rare.
Data from the Mayo Clinic indicates that the real risk of developing muscle pain specifically from the drug's mechanism is about 5% or less compared to placebo. Serious conditions like rhabdomyolysis occur in fewer than 1 case per million person-years. Most observational studies report higher rates of muscle symptoms (up to 20%), but these studies suffer from bias. Patients know they are taking a statin, so they attribute any ache to the drug. Blinded trials, where patients don't know what they are taking, consistently show no difference in subjective symptoms between statins and placebos.
This distinction matters. If you assume every muscle ache is a toxic reaction, you will stop the drug. If you understand that your brain might be amplifying normal sensations, you might give the drug a fair chance. The timing of symptoms also tells a story. In the SAMSON trial, symptoms appeared within days of starting either the statin or the placebo and resolved quickly upon stopping. This rapid onset and offset contradicts the typical timeline of drug-induced tissue damage, further pointing to a central nervous system response rather than cellular injury.
Why Do Statins Trigger This Response More Than Other Drugs?
You might wonder why statins get this reputation while other common medications do not. Several factors converge here. First, statins are long-term preventative treatments. You take them for decades to avoid a heart attack that hasn't happened yet. Unlike antibiotics that cure an immediate infection, statins offer invisible protection. This lack of immediate positive feedback makes patients hyper-aware of any negative sensation.
Second, the media coverage of statin side effects has been intense. Headlines warning of "muscle pain" and "memory loss" create a strong narrative. Dr. Robert Giugliano, a cardiovascular specialist at Harvard Medical School, noted that clinicians should not interpret symptom timing as proof of causation because the pattern is identical for placebos. Yet, patients read these warnings and internalize them. A strong predictor of whether you will experience muscle aches is simply whether you have read about them before starting the medication.
Third, statins are often prescribed alongside lifestyle changes. Diet shifts, increased exercise, and weight management can all cause temporary muscle soreness. Without a blinded control, patients naturally blame the new pill rather than the new gym routine or the change in diet.

How Doctors Are Changing Their Approach
The medical community is waking up to this reality. Major organizations like the American College of Cardiology and the American Heart Association have updated their guidelines to incorporate nocebo awareness. The goal is not to dismiss patients' concerns but to empower them with data.
Clinicians are now adopting specific strategies to help patients stay on therapy:
- Educational Counseling: Before prescribing, doctors explain the nocebo effect. They tell patients, "Your brain might try to trick you into feeling pain. Here is why that happens." This pre-emptive framing reduces the power of the expectation.
- Start Low, Go Slow: Instead of high doses, doctors may start with low-dose atorvastatin (10 mg) or rosuvastatin (5 mg). Lower doses reduce the likelihood of true side effects and build confidence.
- Personalized Tracking: Inspired by the SAMSON trial, some clinics use apps to track symptoms. Seeing objective data that shows symptoms fluctuating regardless of the pill helps patients realize their perception was skewed.
- Reintroduction Protocols: For those who quit, a structured reintroduction plan is offered. Surveys show that clinicians who educate patients about the nocebo effect see restart rates jump from 22% to nearly 49%.
This shift represents a move toward shared decision-making. It acknowledges that while the drug is chemically inert regarding pain for most, the patient's experience is valid. By addressing the psychological component, doctors can preserve the physical benefits of cholesterol lowering.
What Should You Do If You Feel Side Effects?
If you are currently taking statins and experiencing discomfort, do not stop abruptly. Sudden discontinuation can raise your cardiovascular risk. Instead, consider these steps:
- Talk to Your Doctor: Share your symptoms openly. Ask if they could be related to the nocebo effect. Request a review of your dosage or formulation.
- Rule Out Other Causes: Ensure your muscle pain isn't coming from vitamin D deficiency, thyroid issues, or overexertion. Blood tests for CPK (creatine phosphokinase) can confirm if there is actual muscle damage. Normal CPK levels suggest the pain is not due to tissue destruction.
- Consider a Washout Period: Under medical supervision, you might stop the statin for a few weeks to see if symptoms resolve completely. Then, restart with a low dose. If symptoms return immediately despite low doses, discuss alternative lipid-lowering therapies.
- Explore Alternatives: If you truly cannot tolerate statins, options exist. PCSK9 inhibitors like Repatha are injectable drugs that lower cholesterol through a different mechanism and may bypass the nocebo association entirely. Bempedoic acid is another oral option that acts differently in the body.
Remember, the goal is heart protection. Whether you achieve that through statins, alternatives, or intensive lifestyle changes, staying engaged with your healthcare provider is key. The nocebo effect is powerful, but knowledge is stronger. By understanding how your mind influences your body, you can take control of your treatment plan.
Is the nocebo effect dangerous?
The nocebo effect itself is not physically damaging like a toxin, but it is dangerous indirectly. It causes patients to stop effective preventive medications like statins. This leads to higher rates of heart attacks, strokes, and other cardiovascular events that could have been avoided. The danger lies in the loss of protection, not the symptom generation.
Can I distinguish between real side effects and nocebo?
On your own, it is very difficult because the pain feels identical. The only way to distinguish them reliably is through a blinded trial or careful medical monitoring. If blood tests like CPK are normal and symptoms appear rapidly after starting the drug (or even a placebo), it is likely nocebo. True muscle damage usually presents with elevated enzymes and progressive weakness.
Does the SAMSON trial apply to all statins?
The SAMSON trial specifically tested atorvastatin. However, the mechanism of the nocebo effect is psychological, not chemical, so it applies to the entire class of statins. Patients who react negatively to one statin due to expectation often react similarly to others unless the psychological trigger is addressed.
Should I ignore my doctor's warnings about side effects?
No. You should listen to them, but understand the context. Doctors are required to inform you of risks. However, modern guidance emphasizes that while risks exist, they are rare for serious issues and often exaggerated for subjective ones like muscle aches. Use the information to monitor yourself, not to fear the medication.
Are there supplements that help with statin side effects?
Coenzyme Q10 (CoQ10) is often suggested, as statins can deplete CoQ10 levels. While evidence is mixed, some patients report reduced muscle pain with supplementation. However, if your pain is driven by the nocebo effect, supplements will not help. Addressing the expectation of pain is more effective than trying to counteract a chemical deficit that may not exist.