
You might have heard that finding a polyp during a colonoscopy is bad news. But here is the thing: finding them is actually good news. It means you caught something before it could become cancer. The tricky part isn't just knowing what a polyp is-it's understanding which type you have and why it matters for your future health. Not all polyps are created equal. Some are lazy bystanders, while others are sneaky troublemakers that hide in plain sight.
For decades, doctors focused almost exclusively on one type of growth called an adenoma, which is a common precancerous growth in the colon that follows a well-understood pathway to cancer. We knew how to spot them, remove them, and predict their behavior. But then, another player entered the stage: the serrated lesion, which is a distinct category of polyps with a saw-tooth appearance under a microscope that causes a significant portion of colon cancers. These are different beasts. They grow differently, they hide better, and they follow a completely different biological roadmap to malignancy. Understanding the difference between these two groups is the key to staying ahead of colorectal cancer.
The Old Guard: Understanding Adenomatous Polyps
Let’s start with the most familiar face in the room. Adenomas account for about 70% of all polyps found during screenings. Think of them as the conventional suspects. Doctors have been studying them since the 1980s, so we know their playbook inside out. They don’t appear overnight; it usually takes 10 to 15 years for an adenoma to transform into cancer if left alone. That long window is exactly why screening works so well.
Adenomas aren’t a single monolith; they come in three main shapes, each with its own risk profile:
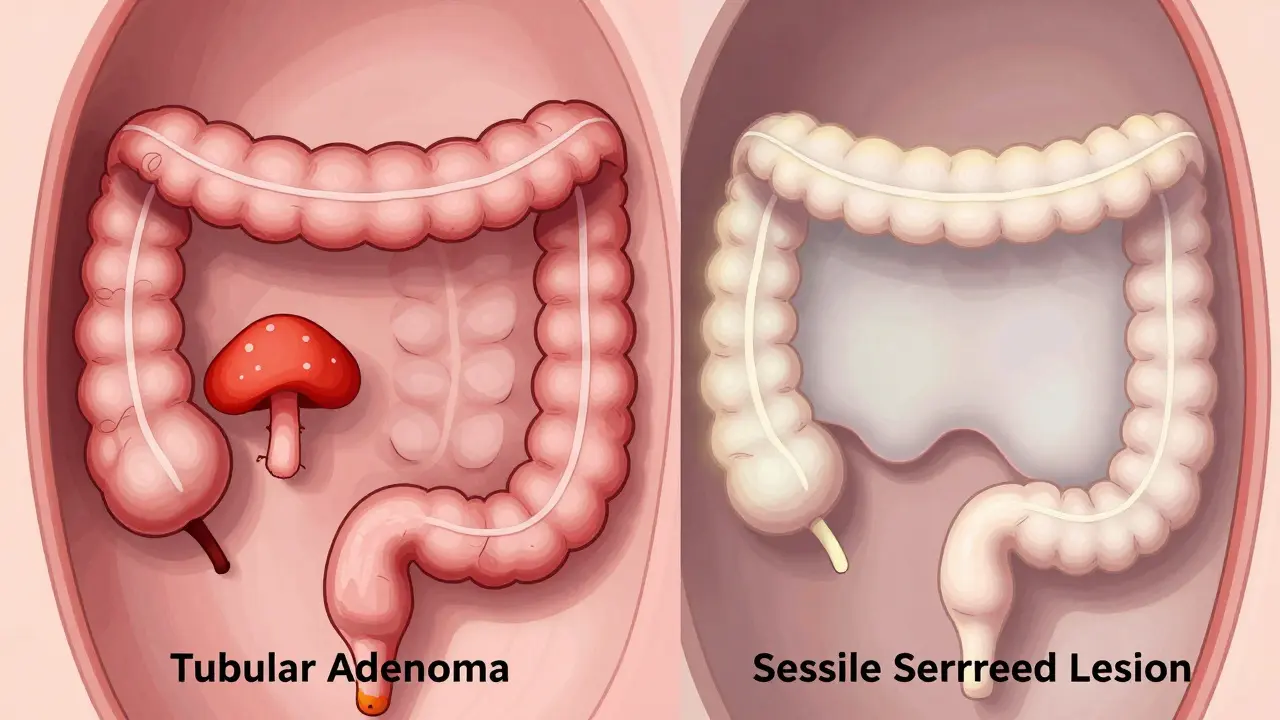
- Tubular adenomas: These are the most common, making up roughly 70% of adenomas. They look like tiny tubes under a microscope. While they are still precancerous, they carry the lowest risk among the adenoma family.
- Tubulovillous adenomas: As the name suggests, these are a mix of tubular and villous features. They represent about 15% of cases and sit in the middle ground regarding risk.
- Villous adenomas: These are the ones to watch closely. Making up the remaining 15%, they often feel velvety or flat against the colon wall. They are harder to remove completely and have a much higher chance of already containing cancer cells.
Size matters immensely here. If you have a small adenoma-say, smaller than half an inch (1.27 cm)-the odds of it harboring cancer are less than 1%. But once an adenoma grows larger than 1 centimeter, that risk jumps to 10-15%. Villous components add another layer of danger, increasing cancer risk by 25-30% compared to purely tubular ones of the same size. The good news? Most adenomas stick out from the wall like little mushrooms (pedunculated) or broad-based bumps (sessile), making them relatively easy for a skilled endoscopist to see and snip off.
The Sneaky Intruders: Serrated Lesions
Now, let’s talk about the group that has changed the game in recent years. Serrated lesions get their name from their jagged, "saw-tooth" appearance when viewed under a microscope. For a long time, doctors dismissed some of these as harmless hyperplastic polyps. We were wrong. Today, we know that serrated lesions cause between 20% and 30% of all colon cancers. That is a massive number, and it explains why early-onset colorectal cancer rates are ticking upward despite better screening for traditional adenomas.
Serrated lesions fall into three categories, and distinguishing between them is critical:
- Hyperplastic polyps: These are generally benign, especially if they are small and located in the lower colon (rectum or sigmoid). You can think of them as the "innocent bystanders" of the serrated world.
- Sessile Serrated Adenomas/Polyps (SSA/Ps): This is the big concern. SSA/Ps are flat, pale, and often blend seamlessly with the surrounding tissue. They love the proximal colon-the upper part near the cecum-which is the hardest area to clean and inspect during a colonoscopy. A study published in Colorectal Disease showed that SSA/Ps have a malignant potential equivalent to conventional adenomas, with high-grade dysplasia or carcinoma present in 13% of cases.
- Traditional Serrated Adenomas (TSAs): These are rarer but aggressive. They often contain dysplasia (abnormal cell growth) at the time of discovery and require careful removal.
The real danger with SSA/Ps is their stealth mode. Unlike adenomas that bulge outward, SSA/Ps are often inverted or flat-elevated. During a standard colonoscopy, they can look like a fold in the lining or a bit of stool residue. The miss rate for sessile polyps hovers around 2-6%, but for subtle serrated lesions, it can be higher if the doctor isn’t specifically looking for them using advanced imaging techniques.
Head-to-Head: How They Differ Biologically
Why does this distinction matter beyond just naming conventions? Because they take different roads to hell. Your body doesn’t just randomly develop cancer; it follows specific genetic pathways. Knowing which pathway is active helps doctors decide how aggressively to monitor you.
| Feature | Adenomas (Conventional) | Serrated Lesions (SSA/Ps) |
|---|---|---|
| Molecular Pathway | Chromosomal Instability (APC gene mutation) | CpG Island Methylator Phenotype (BRAF mutation) |
| Typical Location | Left side (descending/sigmoid colon) | Right side (cecum/ascending colon) |
| Appearance | Bumpy, mushroom-like, or broad-based | Flat, pale, invisible folds, or sticky mucus |
| Detection Difficulty | Moderate (visible with standard light) | High (requires magnification or AI assistance) |
| Risk Profile | Predictable progression over 10-15 years | Can progress faster; insidious due to flat shape |
This biological split is crucial. Adenomas usually involve mutations in the APC gene, leading to chromosomal instability. Serrated lesions, particularly SSA/Ps, often involve BRAF mutations and epigenetic silencing (methylation). This means that even if you clear out all the adenomas today, you could still be at risk for cancer developing via the serrated pathway tomorrow if those flat lesions were missed or if new ones form.
The Detection Challenge: Why Miss Rates Happen
You might wonder, "If my doctor did a thorough job, why would I miss anything?" Colonoscopy is highly effective, but it is not perfect. Human eyes can tire, and the colon is a complex, folded tube. The biggest enemy of detection is preparation. If your bowel isn’t perfectly clean, a flat, pale SSA/P can hide behind a drop of brown fluid.
But even with a clean prep, morphology plays a huge role. Pedunculated polyps (on stalks) are easy targets. Sessile serrated lesions are not. They lie flat. In fact, research indicates that 68.4% of SSA/Ps are located in the proximal colon, far away from the rectum where the scope enters. By the time the doctor reaches that deep, the water and air used to inflate the colon can obscure vision, and the natural folds of the right colon create blind spots.
This is where technology is stepping in. Recent advances include AI-assisted systems like GI Genius, which received FDA approval in 2022. These tools act as a second pair of eyes, highlighting suspicious areas in real-time. Clinical trials published in The Lancet Gastroenterology & Hepatology showed these systems increased adenoma detection rates by 14-18%. More importantly for our discussion, they are showing promise in catching those elusive serrated lesions that human eyes might skip over.
Surveillance: What Comes Next?
So, you had a colonoscopy. They found a polyp. They removed it. Now what? The answer depends entirely on what the pathologist says was removed. This is where guidelines sometimes diverge, causing confusion for patients.
If you had a few small tubular adenomas, you might be told to come back in 5 to 10 years. That sounds relaxing, but it assumes your risk is low. However, if you had a large villous adenoma, or multiple adenomas, that interval shrinks to 3 years. Here is where serrated lesions complicate things. The US Multi-Society Task Force on Colorectal Cancer recommends 3-year surveillance for patients with SSA/Ps larger than 10mm. Why so soon? Because the risk of recurrence or new growth is higher, and the consequences of missing another flat lesion are severe.
Interestingly, European guidelines from the European Society of Gastrointestinal Endoscopy suggest a 5-year interval for similar findings, citing lower observed progression rates in European populations. This discrepancy highlights that medicine is not always black and white. Your gastroenterologist will weigh your personal history, family genetics, and the specific pathology report to give you a tailored plan.
Dr. Matthew Kalady from Ohio State University notes that the serrated pathway accounts for 15-30% of all colorectal cancers, with SSA/Ps being "particularly insidious." This means that if you have a history of serrated lesions, you cannot afford to be complacent. Regular screenings are non-negotiable.

Proactive Steps for Patients
Knowledge is power, but action saves lives. Here is how you can advocate for yourself during your next screening:
- Ask about quality metrics: Don’t be shy. Ask your provider about their Adenoma Detection Rate (ADR). A high-quality colonoscopy should find adenomas in at least 25-30% of average-risk adults. If the rate is lower, you might want a second opinion.
- Insist on a clean prep: Follow the bowel prep instructions to the letter. A messy colon is a missed polyp waiting to happen. Clear liquid diets and proper hydration make a huge difference.
- Request advanced imaging: If available, ask if your center uses Narrow Band Imaging (NBI) or AI-assisted detection. These technologies enhance the contrast of blood vessels and surface patterns, making flat serrated lesions pop out visually.
- Understand your pathology: When you get your results, don’t just look for the word "polyp." Look for the subtype. Was it tubular? Villous? Sessile serrated? Hyperplastic? Write it down. This determines your next appointment date.
- Watch for symptoms: While most polyps are silent, pay attention to rectal bleeding, iron deficiency anemia, or persistent changes in bowel habits. If you experience these, don’t wait for your scheduled screen.
Remember, Dr. Elizabeth Platz from Johns Hopkins puts it plainly: "Most patients with these polyps never develop cancer." The goal of screening is to keep you in that "never" category. By removing the precursors, you break the chain of events that leads to malignancy.
The Future of Polyp Detection
We are standing on the brink of a new era in gastrointestinal care. The days of relying solely on the naked eye are fading. The American Gastroenterological Association predicts that within five years, molecular characterization of polyps will become standard practice. Imagine having a biopsy analyzed not just for its shape, but for its DNA methylation status. If a polyp shows signs of rapid progression markers, you get monitored more closely. If it’s stable, you go home with peace of mind. This personalized approach could reduce the millions of unnecessary surveillance colonoscopies performed annually.
Furthermore, the rise in early-onset colorectal cancer among adults under 50 is alarming. SEER data shows a 2% annual increase in incidence in this demographic. Researchers are now investigating whether environmental factors, diet, or microbiome changes are driving this shift, particularly through the serrated pathway. Until we have clearer answers, lowering the screening age and maintaining rigorous surveillance protocols is our best defense.
Whether you have adenomas or serrated lesions, the message remains the same: detection is victory. These growths are warnings, not sentences. By understanding the differences, demanding high-quality care, and adhering to your surveillance schedule, you take control of your gut health. Don’t let fear stop you from getting screened. Let knowledge empower you to stay healthy.
What is the difference between an adenoma and a serrated polyp?
The primary difference lies in their microscopic appearance and biological pathway. Adenomas have glandular structures and typically follow the chromosomal instability pathway (APC mutation). Serrated polyps have a jagged, saw-tooth pattern and often follow the CpG island methylator phenotype pathway (BRAF mutation). Serrated lesions, particularly sessile serrated adenomas, are flatter and harder to detect than typical adenomas.
Are all serrated polyps precancerous?
No. Hyperplastic polyps, a type of serrated lesion, are generally benign, especially if small and located in the lower colon. However, sessile serrated adenomas/polyps (SSA/Ps) and traditional serrated adenomas (TSAs) are considered precancerous and require complete removal and close monitoring.
How often should I get a colonoscopy if I have serrated lesions?
Guidelines vary, but the US Multi-Society Task Force recommends a 3-year surveillance interval for patients with sessile serrated lesions larger than 10mm. Smaller lesions or those fully removed may allow for longer intervals, but this decision should be made by your gastroenterologist based on your specific pathology report.
Why are serrated lesions harder to detect?
Serrated lesions, especially SSA/Ps, are often flat or slightly depressed rather than raised. They tend to be pale and blend in with the normal colon lining. They also frequently occur in the right side of the colon (proximal), which is harder to visualize thoroughly due to bowel folds and preparation quality.
Can lifestyle changes prevent polyps?
While no guarantee exists, evidence suggests that a diet high in fiber, fruits, and vegetables, combined with regular physical activity and avoiding smoking and excessive alcohol, can reduce the risk of developing both adenomas and serrated lesions. Maintaining a healthy weight is also a significant protective factor.
What does "high-grade dysplasia" mean in a polyp report?
High-grade dysplasia means the cells in the polyp look very abnormal and are close to becoming cancerous. It is a serious finding that requires complete removal of the polyp and often shorter surveillance intervals. It does not necessarily mean you have cancer, but it indicates a high risk if left untreated.